On a bit of an ApoB roll here this eve. It is such an annoying associational variable, that scares the poor low carbers who come in high. We’ll put aside the actual data, which suggests that ApoB is a poor indicator for LCHF low-IR people. Based on logic, why might the high number be irrelevant for low-IR LCHF types? Think about it for a moment:
1. For NON Insulin Resistant (NON Metabolic Syndrome) people, there is good concordance between LDLc and LDLp. High LDLc generally goes with high LDLp. We now know that LDLc is bullshit biometric, with essentially no meaning outside of the hyperinsulinemic hordes. So we can forget LDLp for these non-IR people also, along with the risible LDLc.
2. For Insulin Resistant Met Syn peeps, there is discordance between LDLc and LDLp. Thus you can have low LDLc with high LDLp. The high LDLp now becomes an excellent reflector of Insulin Resistance itself. So you gotta watch the LDLp in this scenario – it now associates strongly with heart events. (the farcical LDLc is of course worse than useless here). But hold on a minute – in these IR people the LDLp is acting as a surrogate for IR – so why the hell would you use this devious metric for Low-IR LCHF peeps?
Whether 1. or 2. above, LDLp is the associational variable from hell. What a goddamn mess… 🙂
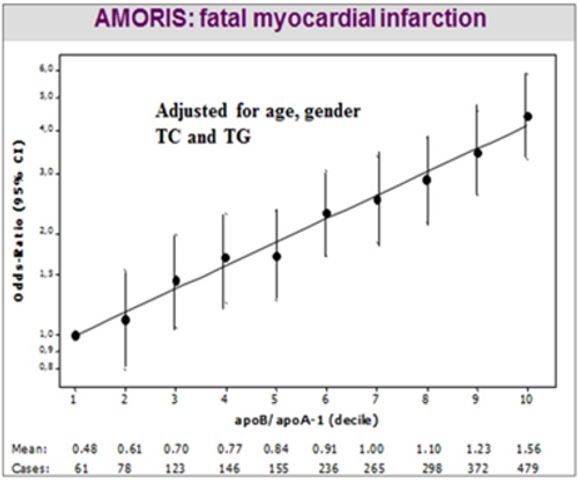
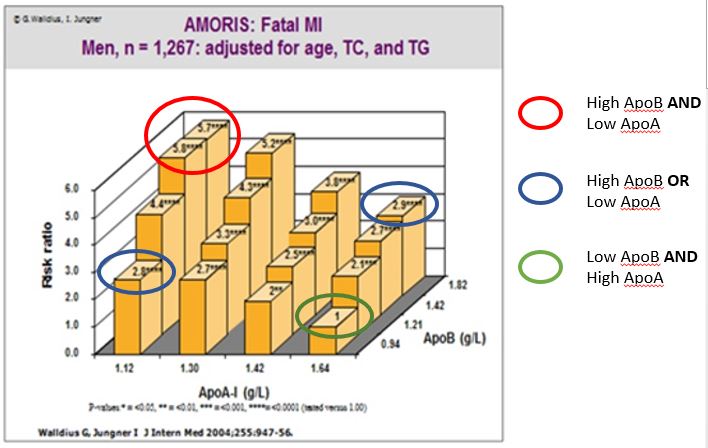
p.s.We haven’t even mentioned ApoA1 here. If anything, ApoB/ApoA1 is the only metric that should be looked at – it is far more powerful than ApoB alone. Of course healthy LCHF peeps with high ApoB will generally have a good ApoB/ApoA1 ratio. Dum de dum…what sleight of hand this particle-count trickery really is…!
From the great AMORIS Study, with nearly 180,000 people tracked across many countries: http://www.ncbi.nlm.nih.gov/pubmed/11755609 . Only a devious idiot would use ApoB rather than ApoB/ApoA1. It’s a joke: